Myopia Control - Overview and Current Treatments

What is myopia?
Myopia, or shortsightedness, is a common condition where objects in the distance appear blurry. It often develops in childhood and may progress as children grow. Myopia progression refers to the continuous increase in the degree of myopia over time, commonly observed in children and adolescents. This progression is largely driven by the elongation of the eye's axial length. The rate at which myopia progresses can vary significantly depending on factors like genetics, environmental influences, and visual habits.
Why Myopia Progression is a Concern
There is growing evidence linking progressive myopia to serious eye health risks such as retinal detachment, glaucoma, and myopic maculopathy later in life. With increasing prevalence of myopia globally, especially in children, it has become critical to slow its progression to reduce these long-term complications. Advances in treatment options, such as orthokeratology (ortho-K), soft multifocal contact lenses, atropine eye drops, and lifestyle modifications like increased outdoor time, have proven effective in managing myopia progression.
International Myopia Institute (IMI) white papers provides evidence-based guidance on myopia control - it emphasizes the need to transition from merely correcting short sightedness with regular glasses or contact lenses, to proactively managing myopia progression and protecting the eye health in the long term.
Myopia control is now considered the standard of care.
Current Treatments for Myopia Progression
Myopia control strategies, like the use of low-dose atropine, multifocal contact lenses, and orthokeratology (ortho-K), aim to reduce the rate of eye elongation, thereby reducing the risks associated with high myopia. When comparing myopia treatments, we consider the effectiveness of the treatment, patient suitability, any side effects and how well it fits into the patient’s lifestyle.

Orthok
Lifestyle Adjustments:
Increasing outdoor time to at least two hours per day has been shown to reduce the risk of myopia development. Additionally, managing screen time and encouraging breaks from close-up activities like reading can help mitigate myopia progression.
Atropine Eye Drops
Efficacy: Atropine is highly effective, particularly at concentrations of 0.05%, which has been shown to slow myopia progression by up to 50%. Lower doses (0.01%-0.025%) are still effective but less so, with fewer side effects.
Ease of Use: Atropine drops are applied once daily, typically at night. While the application itself is straightforward, using eye drops consistently requires compliance. Some children may experience mild side effects like light sensitivity or difficulty reading up close, which can be managed with glasses
2. Orthokeratology (Ortho-K)
Efficacy: Ortho-K lenses, worn overnight, have been shown to reduce myopia progression by around 40-50%. They reshape the cornea temporarily, providing clear vision during the day and slowing eye growth.
Ease of Use: While Ortho-K lenses eliminate the need for daytime glasses or contacts, they require nightly wear and careful cleaning. Most children adapt well to these routines.
3. Multifocal Contact Lenses
Efficacy: Multifocal soft contact lenses (such as MiSight) can slow myopia progression by around 40-50%. They create different focal zones on the retina, which helps reduce the stimulus for eye elongation.
Ease of Use: These lenses are worn during the day, and they require good hygiene and care. Some children might find them more convenient than glasses, especially for sports and active play.
4. Myopia Control Spectacle Lenses
Efficacy: Newer designs like Myosmart spectacle lenses have been found to slow myopia progression by around 40-50%. This option is particularly beneficial for children who are not comfortable with contact lenses(
Ease of Use: Spectacle lenses are easy to use and familiar for most children. They are a non-invasive option, but some children might find wearing glasses limiting, especially during sports or outdoor activities.
Combination therapy
Atropine + Ortho-K: One of the most effective combinations, this approach can significantly reduce myopia progression beyond what either treatment can achieve alone
Atropine + Multifocal Soft Contact Lenses: This combination is also promising, especially for children who prefer soft lenses over wearing Ortho-K lenses at night.
Lifestyle + Any Treatment: Adding more outdoor time and managing screen use can improve the effectiveness of any primary treatment.
While these treatments can slow the progression of myopia, they do not cure or reverse it. The key is early diagnosis and a combination of treatments to protect long-term eye health.
Undercorrection and myopia progression
Studies have shown that undercorrecting myopia can actually accelerate the progression of the condition. This is because undercorrection may cause increased retinal defocus, where the light is focused behind the retina when looking at distant objects. This defocus may stimulate further elongation of the eye, thereby worsening myopia.
Current myopia management strategies aim to control eye growth using full correction and treatments like multifocal lenses, orthokeratology, or atropine eye drops, which focus on providing accurate vision correction while managing the underlying myopia progression
Myopia management guidelines best practice
Infographic below shows evidence based recommendations from Myopia Profile. Up to date as of 2024.
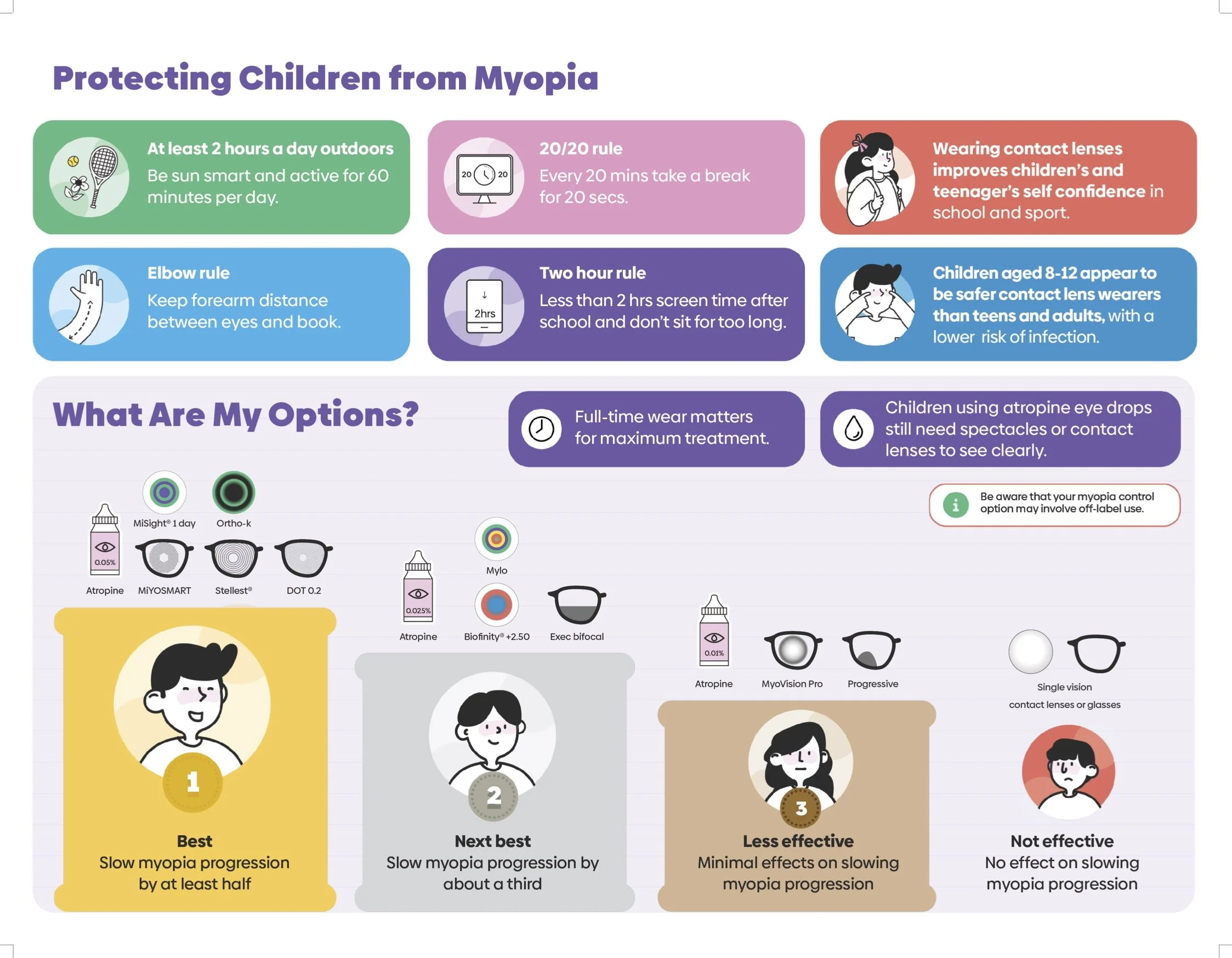
Image courtesy of Myopia Profile and MyKidsVision, https://www.mykidsvision.org/knowledge-centre/understanding-the-myopia-profile-infographic
How can we determine whether treatments are working effectively
To determine if myopia control treatments like Orthok, soft multifocal lenses, or atropine drops are working, several key indicators can be monitored:
Stabilization of Prescription: The most reliable way to tell if myopia control is effective is by tracking changes in the patient's prescription over time. A slowing or stabilization of myopic progression, indicated by smaller increases in diopters (less change in shortsightedness), suggests the treatment is working. Optometrists typically measure refractive changes during regular follow-up visits.
Axial Length Measurement: Another critical factor is the axial length of the eye, which increases as myopia worsens. Slower growth of the axial length, measured by devices such as an optical biometer, is a strong indicator that the treatment is effectively controlling myopia progression(
Vision Quality: Patients should maintain stable, clear vision with fewer fluctuations throughout the day. If the quality of vision is consistently good and does not deteriorate rapidly, it is a positive sign that myopia control is functioning as intended.
Annual Progression Comparisons: For children and teenagers, annual comparisons are useful. Myopia progression is typically fastest in younger children, so if the progression rate is reduced compared to age-expected rates or previous years, it is a sign of effective myopia control. The chart below gives an example of what an optometrist may use to gauge success.

Image courtesy of Myopia Profile and MyKidsVision, https://www.mykidsvision.org/knowledge-centre
FAQs
Can my child’s myopia be treated with laser surgery?
Laser surgery, such as LASIK, is not recommended for children or teenagers because their eyes are still growing. Additionally, while laser surgery can correct the refractive error, it does not slow down any progression or reduce the underlying risk of eye conditions associated with high myopia.
What is the best age to start myopia control treatment?
Myopia control treatments are most effective when started as early as possible, typically around the age of 6 to 8 years, when the eye is still growing rapidly. Treatments are usually recommended throughout childhood and adolescence, until eye growth stabilizes.
Can combination therapy improve myopia control?
Yes, combination therapy (e.g., using atropine drops with Ortho-K lenses) can enhance the effectiveness of myopia control. Studies show that combining treatments can achieve better results than using a single method, offering greater reductions in myopia progression.
How often should my child have eye check-ups if they have myopia?
Children with myopia should have regular eye check-ups, typically every 6-12 months, to monitor progression and adjust treatments as needed. Early and consistent management ensures better outcomes.
Are there any risks associated with myopia treatments?
Most myopia treatments are safe and well-tolerated. Atropine eye drops can cause mild side effects such as light sensitivity or difficulty with near vision, while Ortho-K lenses require proper hygiene to avoid infections. Your eye care professional will monitor for any side effects during regular follow-ups.
Does computer use increase the risk of myopia progression?
Yes, excessive computer use, especially at close distances, can increase the risk of myopia progression. Studies suggest that prolonged near work, such as using computers or other digital devices, places strain on the eyes, which may lead to myopia or worsen existing myopia. Encouraging regular breaks (using the 20-20-20 rule: every 20 minutes, look at something 20 feet away for 20 seconds) and ensuring that screens are kept at a proper distance can help manage this risk
Is myopia inherited?
Yes, genetics play a significant role in the development of myopia. If one or both parents have myopia, their children are at a higher risk of developing the condition. However, environmental factors, such as time spent outdoors and near work activities, also contribute to the onset and progression of myopia
When does myopia progression typically slow down
Myopia progression typically slows down by the late teenage years to early adulthood. Most commonly, myopia progression stabilizes around ages 18 to 21, when the eye's growth naturally slows or stops. However, for some individuals, myopia may continue to progress.
Factors such as genetics, lifestyle, and the initial onset age of myopia can influence when it stabilizes. Children who develop myopia earlier (before age 8) tend to have a longer period of progression compared to those who develop it later.
How can we estimate risk of myopia progession in my child?
Go to the MyKidzVision risk calculator to assess risk. https://www.mykidsvision.org/en-US/risk-assessment
Make it stand out
Whatever it is, the way you tell your story online can make all the difference.
Image courtesy of Myopia Profile and MyKidsVision, https://www.mykidsvision.org/knowledge-centre/understanding-the-myopia-profile-infographic
References
Flitcroft DI. The complex interactions of retinal, optical and environmental factors in myopia aetiology. Prog Retin Eye Res. 2012 Nov;31(6):622-60.
Bullimore MA, Brennan NA. Myopia Control: Why Each Diopter Matters. Optom Vis Sci. 2019 Jun;96(6):463-465.
Jonas JB, Ang M, Cho P, Guggenheim JA, He MG, Jong M, Logan NS, Liu M, Morgan I, Ohno-Matsui K, Pärssinen O, Resnikoff S, Sankaridurg P, Saw SM, Smith EL 3rd, Tan DTH, Walline JJ, Wildsoet CF, Wu PC, Zhu X, Wolffsohn JS. IMI Prevention of Myopia and Its Progression. Invest Ophthalmol Vis Sci. 2021 Apr 28;62(5):6.
Tahhan N, Wolffsohn JS, Sankaridurg P, Jonas JB, Bullimore MA, Flitcroft I, et al. International Myopia Institute White Paper Series 2023. Invest Ophthalmol Vis Sci. 2023;64(6):1. doi: https://doi.org/10.1167/iovs.64.6.1
The impact of myopia and high myopia. Report of the Joint World Health Organization-Brien Holden Vision Institute Global Scientific Meeting on Myopia. 2015.
Tang Y, Wang X, Wang J, Huang W, Gao Y, Luo Y, Lu Y. Prevalence and Causes of Visual Impairment in a Chinese Adult Population: The Taizhou Eye Study. Ophthalmology. 2015 Jul;122(7):1480-8.
Gifford KL, Richdale K, Kang P, Aller TA, Lam CS, Liu YM, Michaud L, Mulder J, Orr JB, Rose KA, Saunders KJ, Seidel D, Tideman JWL, Sankaridurg P. IMI - Clinical Management Guidelines Report. Invest Ophthalmol Vis Sci. 2019 Feb 28;60(3)
MyKidz Vision. Myopia Information and Resources for Parents and Professionals. MyKidz Vision
Author Bio
Jenny Wu is an optometrist based in Canberra, Australia. She is a full scope optometrist specializing in dry eye, specialty contact lenses, myopia control, and orthok. She practices at Simpson Optometry. In her spare time she enjoys spending time in nature, photography, gardening, and being with her husband (also an optometrist) and 2 children.